This section focusses on the internal
female reproductive organs: the ovaries, oviducts, uterus and
vagina. We will also have a look at the mammary gland, an accessory reproductive gland.
The external female genitalia include the labia minora and majora,
clitoris and vestibule. Their structures
are part of HA235 Anatomy.
The ovaries have two functions -
"production" and ovulation of oocytes and the production and
secretion of hormones. The ovary is attached to the broad
ligament by a short fold of peritoneum, called the mesovarium (or ligament
of the ovary), through which vessels and nerves pass to the
ovary and enter it at the hilus of the ovary.
The surface of the ovary is covered by a single layer of cuboidal epithelium,
also called germinal epithelium. It is continuous
with the peritoneal mesothelium. Fibrous connective tissue forms a thin capsule,
the tunica albuginea, immediately beneath the
epithelium.
Like so many other organs the ovary is divided into an outer
cortex and an inner medulla. The cortex consists of a very cellular
connective tissue stroma in which the ovarian follicles are
embedded. The medulla is composed of loose connective tissue, which
contains blood vessels and nerves.
Ovarian follicles consist of one oocyte and surrounding follicular
cells. Follicular development can be divided into a number of stages.
Development represents a morphological
continuum, and it may not be possible to assign all follicles to a specific stage. This said,
it's pretty easy most of the time.
- Primordial
follicles
-
are located in the cortex just beneath tunica albuginea. One layer of
flattened follicular cells surround the oocyte (about
30 µm in diameter). The nucleus of the oocyte is positioned
eccentric in the cell. It appears very light and contains a prominent
nucleolus.
Most organelles of the oocyte aggregate in
the centre of the cell, where they form the vitelline body (probably not visible in any of
the available preparations).
- The primary
follicle
-
is the first morphological stage that marks the onset of
follicular maturation (Which hormone
stimulates follicular maturation? Where is this hormone
produced?). The previously flattened cell surrounding
the oocyte now form a cuboidal or columnar epithelium surrounding
the oocyte. Their cytoplasm may have a granular appearance, and
they are for this reason also called
granulosa cells. The continued proliferation of these cells
will result in the formation of a stratified epithelium (with a
distinct basement membrane) surrounding the oocyte. The zona pellucida (glycoproteins between
interdigitating processes of oocyte and granulosa cells) becomes
visible. Parenchymal cells of the ovary surrounding the growing
follicle become organised in concentric sheaths, the theca folliculi.
- Secondary
follicle
-
Small fluid-filled spaces become visible between the granulosa
cells as the follicle reaches a diameter of about 400 µm.
These spaces enlarge and fuse to form the
follicular antrum, which is the defining feature of the
secondary follicle. The oocyte is now located eccentric in the
follicle in the cumulus oophorus,
where it is surrounded by granulosa cells. The theca folliculi
differentiates with the continued growth of the follicle into a
theca interna and a theca externa. Vascularization of the theca
interna improves, and the spindle-shaped or polyhedral cells in
this layer start to produce
oestrogens. The theca externa retains the characteristics of
a highly cellular connective tissue with smooth muscle cells. The
oocyte of the secondary follicle reaches a diameter of about 125
µm. The follicle itself reaches a diameter of about 10-15
mm.
- The mature or
tertiary or preovulatory or Graafian follicle
-
increases further in size (in particular in the last 12h before
ovulation). The Graafian follicle forms a small "bump" on the
surface of the ovary, the stigma
(or macula pellucida). The stigma is
characterised by a thinning of the capsule and a progressive
restriction of the blood flow to it. Prior to ovulation the cumulus
oophorus separates from the follicular wall. The oocyte is now
floating freely in the follicular antrum. It is still surrounded by
granulosa cells which form the corona
radiata. The follicle finally ruptures at the stigma and the
oocyte is released from the ovary.
Lab: Slide OVARY
MACAQUE H&E. Identify cortex and medulla at low magnification and
verify the presence of large numbers of blood vessels in the medulla. Now
have a look at the cortex at medium/high magnification. Identify the cuboidal
epithelium covering the ovary and the underlying tunica albuginea. Find a
part of the cortex where you can observe primordial, primary and secondary
follicles.
Draw this section of the cortex with its follicles, the
surrounding theca (if present), connective tissue stroma, tunica albuginea
and epithelium.


Atresia is the name for the degenerative process by which oocytes (and follicles)
perish without having been expelled by ovulation. Only about 400 oocytes ovulate
- about 99.9 % of the oocytes that where present at the time of puberty undergo
atresia. Atresia may effect oocytes at all stages of their "life" - both prenatally
and postnatally. By the sixth month of gestation about 7 million oocytes and
oogonia are present in the ovaries. By the time of birth this number is reduced
to about 2 million. Of these only about 400.000 survive until puberty.
Atresia is also the mode of destruction of follicles whose maturation is
initiated during the cyclus (10-15) but which do not ovulate. Atresia is operating
before puberty to remove follicles which begin to mature during this period
(none of which are ovulated). Given that atresia affects follicles at various
stages of their development it is obvious that the process may take on quite
a variety of histological appearances.
The corpus luteum is formed by both
granulosa cells and thecal cells after ovulation has
occurred. The wall of the follicle collapses into a folded
structure, which is characteristic for the corpus luteum.
Vascularization increases and a connective tissue network is
formed. Theca interna cells and granulosa cells triple in size and
start accumulating lutein (Which hormone stimulates this process?
Where is this hormone produced?) within a few hours after
ovulation. They are now called granulosa
lutein cells and theca lutein
cells and produce
progesterone and
oestrogens.
Hormone secretion in the corpus luteum ceases within 14 days
after ovulation if the oocyte is not fertilised. In this case, the
corpus luteum degenerates into a corpus
albicans - whitish scar tissue within the ovaries.
Hormone secretion continues for 2-3 month after ovulation if
fertilisation occurs.
Lab: Slide
CORP. LUTEUM H&E. Hold the slide
against the light and try to identify the corpus luteum. It appears
as a large (5mm-1cm) rounded but somewhat irregularly shaped
structure in the periphery of the ovary. It stains homogenously
bright red except from a reddish irregular structure at its core.
Now have a look using the low magnification and verify the "folded"
appearance of the tissue forming the corpus luteum. You may be able
to find spots in the periphery of the corpus luteum in which a
fairly thin layer of slightly darker cells surround the otherwise
light red cell forming most of the corpus luteum. The dark cell
represent theca lutein cell the lighter ones are granulosa lutein
cells.
Sketch the corpus luteum and ovary at low
magnification and make shure that the relative size of the corpus
luteum becomes apparent in your sketch. Draw, if possible, a spot
where you can differentiate between theca and granulosa lutein
cells.


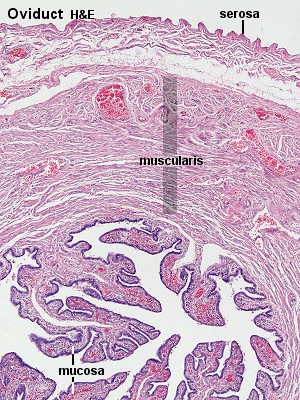
The oviduct functions as a conduit for the oocyte, from the
ovaries to the uterus. Histologically, the oviduct consists of a
mucosa and a muscularis. The peritoneal suface of the oviduct
is lined by a serosa and subjacent connective tissue.
- The
mucosa
-
is fomed by a ciliated and secretory
epithelium resting on a very cellular lamina propria. The
number of ciliated cells and secretory cells varies along the
oviduct (see below). Secretory activity varies during the menstrual
cycle, and resting secretory cells are also referred to as peg-cells. Some of the secreted substances
are thought to nourish the oocyte and the very early embryo.
- The
muscularis
-
consists of an inner circular muscle layer and an outer
longitudinal layer. An inner longitudinal layer is present in the
isthmus and the intramural part (see below) of the oviduct. Peristaltic muscle action seems to be more
important for the transport of sperm and oocyte than the action of
the cilia.
Texts usually refer to four subdivisions of the oviduct.
- The infundibulum is the
funnel-shaped (up to 10 mm in
diammeter) end of the ovdiuct. Finger-like extensions of its
margins, the fimbriae, are closely
applied to the ovary. Ciliated cells are frequent. Their cilia beat
in the direction of
- the ampulla of the oviduct.
Mucosal folds, or plicae, and secondary folds which arise from the
plicae divide the lumen of the ampulla into a very complex shape.
Fertilization usually takes place in the ampulla.
- The isthmus is the narrowest portion
(2-3 mm in diameter) of the parts of the oviduct located in
the peritoneal cavity. Mucosal folds are less complex and the
muscularis is thick. An inner, longitudinal layer of muscle is
present in the istmus and the
- last, intramural part of the
oviduct, which penetrates the wall of the uterus. The term "intramural"
should be familiar to you ..... The mucosa is smooth, and
the inner diameter of the duct is very small.
Oviduct is a nice descriptive term, but
(sigh) not the only one commonly used for these structures -
you will also find the terms Fallopian
tubes or uterine tubes. The
term salpinx (greek, trumpet) seems to have passed its
"use-by-date" in many histology text but
(big sigh) not in pathology, where
salpingitis refers to chronic or acute inflammation of the
oviduct. Let's see how "tubal inflammation"
will fare in the future.
Obstruction of the oviduct as a consequence of salpingitis is
one possible cause of infertility, and alterations of luminal
structure by inflammatory processes are a risk factor for tubal
pregnancies.
Lab: Slide OVARY
MACAQUE H&E (some slides) or UTERUS PROLIF.
PHASE. Unfortunately, we do not have many oviduct slides, but some
sections of the macaque ovary and the uterus slide contains segments of the
oviduct. In the former you should be able to see both the muscularis and the
folded mucosa. Ciliated cells and peg-cells are present. In the intramural
part of the oviduct (uterus slide) the mucosa is smooth and ciliated cells
are rare or absent. The intramural part of the uterus should remind you of a structure
in the male reproductive system - Which one?
Draw part of the wall of the oviduct, identify the segment
and, if possible, ciliated and peg cells.

The uterus is divided into body
(upper two-thirds) and cervix. The walls of the uterus are composed of
a mucosal layer, the endometrium,
and a fibro-muscular layer, the
myometrium. The peritoneal surface of the uterus is covered
by a serosa.
-
Myometrium
-
The muscle fibres of the uterus form layers with prefered
orientations of fibres (actually 4),
but this is very difficult to see in most preparations. The
muscular tissue hypertrophies during pregnancy, and GAP-junctions
between cells become more frequent.
-
Endometrium
-
The endometrium consists of a simple columnar epithelium
(ciliated cells and secretory cells) and an underlying thick
connective tissue stroma. The mucosa is invaginated to form many
simple tubular uterine glands. The
glands extend through the entire thickness of the stroma. The
stromal cells of the endometrium are embedded in a network of
reticular fibres. The endometrium is subject to cyclic changes that
result in menstruation. Only the mucosa of the body of the uterus
takes part in the menstrual cycle.
The endometrium can be divided into two zones based on their
involvement in the changes during the menstrual cycle: the basalis and the
functionalis.
- The basalis is not sloughed off during menstruation but
functions as a regenerative zone for the functionalis after its
rejection.
- The functionalis is the luminal part of the endometrium. It is
sloughed off during every menstruation and it is the site of cyclic
changes in the endometrium. These cyclic changes are divided into a
number of phases: proliferative (or
follicular), secretory (or luteal),
and menstrual (consult Ross et al. for further details).
Lab: Slide
UTERUS PROLIF STAGE H&E. Identify
the muscular wall of the uterus and the endometrium lining the
lumen of the uterus. Identify uterine glands embedded in the stroma
of the endometrium. Finally try to find a
spiral artery. These are arteries ascend through the
endometrium and form a coil/spring like structure while they do so.
How would you expect tis structure to look like in a section?
Sketch a small section of the
endometrium.


The vagina is a fibromuscular tube with a wall consisting of
three layers: the mucosa, muscularis and adventitia of the
vagina
- Mucosa
-
The stratified squamous epithelium (deep stratum basalis,
intermediate stratum spinosum, superficial layers of flat
eosinophilic cells which do contain keratin but which do not
normally form a true horny layer) rests on a very cellular lamina
propria (many leucocytes). Towards the muscularis some vascular cavernous spaces may be seen (typical
erectile tissue).
- Muscularis
-
Inner circular and outer longitudinal layers of smooth muscle
are present. Inferiorly, the striated, voluntary bulbospongiosus
muscle forms a sphincter around the vagina.
- Adventitia
-
The part of the adventitia bordering the muscularis is fairly
dense and contains many elastic fibres. Loose connective tissue
with a prominent venous plexus forms the outer part of the
adventitia.
 Lab: Slide VAGINA HUMAN H&E.
Identify the layers of the vagina. Note that the organization of the wall
of the vagina corresponds in many respects to the organization of the wall
of the oesophagus. It should not be necessary to do a drawing, but compare
your observations in the vagina with those in the oesophagus. Try to define
how the layers differ although they are composed of similar tissue types.
Lab: Slide VAGINA HUMAN H&E.
Identify the layers of the vagina. Note that the organization of the wall
of the vagina corresponds in many respects to the organization of the wall
of the oesophagus. It should not be necessary to do a drawing, but compare
your observations in the vagina with those in the oesophagus. Try to define
how the layers differ although they are composed of similar tissue types.
Female Accessory Reproductive Glands -
Mammary Glands
The mammary glands are modified glands of the skin. Their
development resembles that of sweat glands. They are compound
branched alveolar glands, which consist of 15-25 lobes separated by
dense interlobar connective tissue and fat. Each lobe contains an
individual gland. The excretory duct of each lobe, also called
lactiferous duct, has its own
opening on the nipple.
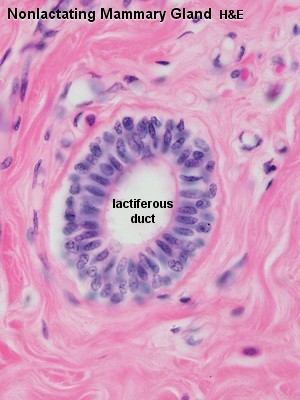
The lactiferous duct has a two layered
epithelium - basal cells are cuboidal whereas the
superficial cells are columnar. Beneath the nipple, the dilated
lactiferous duct forms a lactiferous
sinus , which functions as a reservoir for the milk.
Branches of the lactiferous duct are lined with a simple cuboidal
epithelium. The secretory units are alveoli, which are lined by a
cuboidal or columnar epithelium. A layer of
myoepithelial cells is always present between the epithelium and
the basement membrane of the branches of the lactiferous duct and
the alveoli.
The above description corresponds basically to the appearance of
the resting mammary gland. Pregnancy induces a considerable growth
of the epithelial parenchyma leading to the formation of new
terminal branches of ducts and of alveoli in the first half of
pregnancy. Growth is initiated by the elevated levels of oestrogen
and progesterone produced in the ovaries and placenta.
Concurrently, a reduction in the amount of intra- and interlobular
connective tissue takes place. The continued growth of the mammary
glands during the second half of pregnancy is due to increases in
the height of epithelial cells and an expansion of the lumen of the
alveoli. They contain a protein-rich (large
amounts of immunoglobulins) eosinophilic secretion - the colostrum or foremilk).
Secretion of milk proteins proceeds by exocytosis (merocrine
secretion), whereas lipids are secreted by apocrine secretion.
Secretion is stimulated by
prolactin. Prolactin secretion in turn is stimulated by
sensory stimulation of the nipple, which also initiates the
so-called milk ejection reflex via
the secretion of oxytocin from the
neurohypophysis. Milk is ejected from the glandular tissue into the
lactiferous sinuses - now it's up to the baby to get things
out.
The glandular tissue of
the mammary gland is frequently subject to pathological changes -
the most serious being mammary cancer, which is the most frequent
malignancy in women (about 6.5% of all women develop the
disease).
Lab: Slide
NONLAC BREAST H&E. Identify the
lactiferous ducts. There seem to be two
different types of this slide around - in one of them the
lactiferous ducts are the only visible part of the resting mammary
gland. Try to have a look at slides from other tray - Pleeeaase remember to return the slide to the
right tray. See if you can indetify intercalated ducts and
resting alveoli.
Draw a nice lactiferous duct and, if possible, a
few resting alveoli.
Slide BREAST LACT HUMAN H&E.
Identify the secretory alveoli and interlobular ducts. Do all parts
of the secretory tissue look similar? Why/why not?
Draw and label part of the secretory
tissue.