Blood is sometimes considered to be a fluid connective tissue
because of the mesenchymal origin of its cells and a low ratio of
cells to liquid intercellular substance, the blood plasma. In human adults about 5 l of blood
contribute 7-8 % to the body weight of the individual. The
contribution of red blood cells (erythrocytes) to the total volume of the blood
(haematocrit) is about 43%.
Erythrocytes are the dominant (99%) but not the only type of
cells in the blood. We also find
leucocytes and thrombocytes (blood
platelets). Cells in the blood are also being referred to as
the formed elements of the blood.
Erythrocytes and thrombocytes perform their functions exclusively
in the blood stream. In contrast, leucocytes reside only
temporarily in the blood and leave the blood stream through the
walls of capillaries and venoles and enter either connective or
lymphoid tissues.
Erythrocytes do not contain a nucleus. They do contain
haemoglobin, which fills allmost the entire cytoplasm. They are
nonmotile (they are unable to move actively) but they are
remarkably elastic and can withstand deformation. They are
typically biconcave disks although their shape is influenced by
osmotic forces. The average diameter of the disk is about 7
µm. Since erythrocytes can be found in the vast majority of
histological sections - in small numbers even in perfused tissues -
they will often allow us to estimate the size of other structures
or cells. Mature erythrocytes do not contain organelles, and their
cytoplasm looks fairly homogenous - even in the EM (depending on the magnification some granularity may be
visible. The granular appearance is caused by haemoglobin). Foetal
erythrocytes (up to the 4th month of gestation) are larger than
"adult" erythrocytes. Also, they are nucleated, a feature they
share with erythrocytes of other animal classes (e.g.
birds).
Functions
Erythrocytes function in the transport of oxygen. Haemoglobin,
the oxygen binding protein in erythrocytes, contributes about 30%
of the weight of an erythrocyte. The lifespan of an erythrocyte in
the bloodstream is about 100-120 days.
About 5x1011 erythrocytes are formed/destroyed each
day.
 Lab: Slide BLOOD SMEAR LEISHMAN.
How does the shape of the erythrocyte facilitate its
function? How would you expect an erythrocyte to look like if it is in an
extracellular fluid of very low or very high osmotic pressure?
Lab: Slide BLOOD SMEAR LEISHMAN.
How does the shape of the erythrocyte facilitate its
function? How would you expect an erythrocyte to look like if it is in an
extracellular fluid of very low or very high osmotic pressure?
Identify and draw a few erythrocytes.
It is a good idea to do one large composite drawing for all
types of blood cells.
Leucocytes can be further subdivided into granular (neutrophil,
basophil and eosiniphil) and non-granular (monocytes and
lymphocytes) groups.
In healthy individuals the relative numbers of circulating
leucocyte types are quite stable. A differential leucocyte count would typically produce the following cell frequencies (numbers in parentheses are the range of normal frequencies reported in different texts):
- ~ 60% neutrophils (50% - 70%)
- ~ 3% eosinophils (>0% - 5%)
- ~ 0.5% basophils (>0% - 2%)
- ~ 5% monocytes (1% - 9%)
- ~ 30% lymphocytes (20% - 40%)
Changes in their relative numbers
indicate that something abnormal is happening in the organism. A
larger than usual number of neutrophils
(neutrophilia) would indicate e.g. an acute or chronic
infection. The number of basophils and eosinophils may increase
(eosinophilia or basophilia) as a
consequence of e.g. allergic disorders.
Granular Leucocytes
Granular leucocytes are all approximately the same size - about
12-15 µm in diameter. Their nuclei form lobes (the number of
lobes varies according to cell type), and nucleoli cannot be seen.
All granulocytes are motile.
- Neutrophil
granulocytes (or neurophils)
-
have a very characteristic nucleus. It is divided into 3-5 lobes which are connected by thin strands of
chromatin. The number of lobes is related to cell age (up to
7 lobes in very old neutrophils -
hypersegmented cells).
The term granulocytes refers to the presence of granules
(secretory vesicles) in the cytoplasm of these cells. Specific granules are those granules that are only
found in one particular type of granulocytes.In neutrophils
these granules stain only weakly (if at all visible) - they are
"neutral", hence the term neutrophil. Neutrophils (like all other
granulocytes, monocytes and lymphocytes) contain all the organelles
that make up a typical cell. In addition to the usual complement of
organelles, they also contain two types of granules. Primary
granules (or A granules) contain lysosomal enzymes and are likely
to be primary lysosomes, although they are larger (0.4 µm) than the "ordinary" primary
lysosome. Secondary granules (or B
granules, specific
granules of the neutrophils) contain enzymes with strong
bactericidal actions.
Functions
Neutrophils play a central role in inflammatory processes. Large
numbers invade sites of infection and begin to phagocytose tissue
debris and foreign bodies, e.g. bacteria. They are the first wave
of cells invading sites of infection, and their phagocytotic
activity is stimulated if invading microorganisms are "tagged" with
antibodies. Neutrophils cannot replenish their store of granules,
and they die once their supply has been exhausted. Dead neutrophils
and tissue debris are the major components of pus.
Lost neutrophils are quickly replenished
from a reserve population in the bone marrow. Because they are
younger, their nuclei have fewer lobes than the "average"
neutrophil. A high proportion of neutrophils, with few nuclear
lobes indicates a recent surge in their release from the bone
marrow. Their lifespan is only about one week.
 Lab: Slide BLOOD SMEAR LEISHMAN.
Neutrophil granulocytes are easy to find - they are the most frequent type
of white blood cells. Note that there are apparently two batches (B1 &
B2) of blood smears in the trays. While erythrocytes look very similar in
the two batches, the leucocytes look differently. In B1, neutrophils will
look very pale, and they will not contain any visible granules in their cytoplasm.
In B2, a few very small, dark granules are visible, and the neutrophils generally
stain much stronger.
Lab: Slide BLOOD SMEAR LEISHMAN.
Neutrophil granulocytes are easy to find - they are the most frequent type
of white blood cells. Note that there are apparently two batches (B1 &
B2) of blood smears in the trays. While erythrocytes look very similar in
the two batches, the leucocytes look differently. In B1, neutrophils will
look very pale, and they will not contain any visible granules in their cytoplasm.
In B2, a few very small, dark granules are visible, and the neutrophils generally
stain much stronger.
Have a close look at the nucleus of a
number of neutrophils, and make a qualified guess at the gender of
the individual, which donated blood for the slides.
Identify and draw one or two neutrophil
granulocytes.
- Eosinophil
granulocytes (or eosinophils)
-
Their nucleus usually has only two lobes. Almost all of the
cytoplasm appears filled with the specific granules of the
eosinophils. As the term "eosinophil" indicates, these granules are
not neutral but stain red (or pink) when eosin (or a similar dye)
is used in the staining process. Aside from the usual complement of
organelles eosinophils contain some large rounded granules (up to 1 µm) in their cytoplasm.
These granules correspond to the eosinophilic grains that we see in
the light microscope. The specific granules contain, in addition to
enzymes that otherwise are found in lysosomes, an electron-dense,
laminated, proteinaceous crystal.
Functions
The presence of antibody-antigen complexes stimulates the immune
system. Eosinophils phagocytose these complexes and this may
prevent the immune system from "overreacting". Their granules also
contain the enzyme histaminase,
which breaks down histamine and thus dampens the effects of
vasoactive substances released by basophils or mast cells. The role
of the crystalline inclusion in the granules is somewhat unclear.
The crystal consists of protein, which may
be stored in this form to keep the osmotic pressure down (otherwise
the vesicles would swell and possibly disintegrate). Most
textbooks however agree that the protein and its release by
eosinophils may be involved in the response of the body against
parasitic infections.
Lab: Slide
BLOOD SMEAR LEISHMAN. Eosinophils and
basophils are the only cell types present in normal blood which
initially may be difficult to distinguish. If you see them side by
side in your drawing the difference between them should become
apparent. Basophils are quite rare. Because the populations of
eosinophils and basophils are small (as compared to other
leucocytes) you will very rarely see the two antagonists (Why?) as close together "in the wild" as
on this page AND your drawing. Note that eosinophils and basophils
are much easier to distinguish in B1. In B2, the difference in the
staining of their of granules is not as pronounced, and the nuclei
do not stand out as clear as in B1.
To facilitate your identification of these two
cell types, areas in the blood smear in which at least one good
eosinophil and at least one good basophil are present have been
marked with a red and blue circle respectively. If a circle has a
red and blue outline you should be able to identify both at least
one good basophil and at least one good eosinophil within the
circle.
Identify, draw and label an eosinophil and a
basophil.


- Basophil
granulocytes (or basophils)
-
Basophilic granulocytes have a 2 or 3 lobed nucleus. The lobes
are usually not as well defined as in neutrophilic granulocytes and
the nucleus may appear S-shaped. The specific granules of basophils
are stained deeply bluish (or reddish violet). Their colour corresponds closely (maybe slightly
lighter) to the colour of the nucleus which sometimes is difficult
to see amongst or behind the granules. The granules are not
as numerous as those in eosinophils. The specific granules of
basophils (about 0.5 µm)
appear quite dark in EM pictures. They contain heparin, histamine,
slow-reacting
substance of anaphylaxis
(SRS-A = leukotrienes) and lysosomal
enzymes.
Functions
Heparin and histamine are vasoactive substances. They dilate the
blood vessels, make vessel walls more permeable and prevent blood
coagulation. As a consequence, they facilitate the access of other
lymphocytes and of plasma-borne substances of importance for the
immune response (e.g. antibodies) to e.g. a site of infection. The
release of the contents of the granules of basophils is
receptor-mediated. Basophils do not produce antibodies, but they
bind antibodies produced by plasma cells (activated B-lymphocytes;
see below) on their surface. If these antibodies come into contact
with their antigens, they induce the release of the contents of the
basophil granules.
-
Monocytes
-
These cells can be slightly larger than granulocytes (about 12-18 µm in diameter). Their
cytoplasm stains usually somewhat stronger than that of
granulocytes, but it does not contain any structures which would be
visible in the light microscope using most traditional stains (a few very fine bluish gains may be visible in
some monocytes). The "textbook" monocyte has a
horseshoe-shaped nucleus. Monocytes contain granules (visible in
the EM) which both in appearance and content correspond to the
primary granules of neutrophils.
Functions
Once monocytes enter the connective
tissue they differentiate into macrophages. At sites of
infection macrophages are the dominant cell type after the death of
the invading neutrophils. The phagocytose microorganisms, tissue
debris and the dead neutrophils. Monocytes also give rise to
osteoclasts, which are able to dissolve bone. They are of
importance in bone remodelling.
Lab:
Slide BLOOD SMEAR LEISHMAN . Monocytes
and lymphocytes definitely look much prettier in B2 than in B1 -
mainly because of a clearer distinction between cytoplasm and
nucleus. Note the light area of cytoplasm which is often found
close to the concave surface of the monocyte nucleus. The Golgi
apparatus is located in the area. The Golgi
apparatus does not stain as well as the remainder of the cytoplasm
and leaves a light "impression" - the phenomenon is also called a
"negative image".
Identify and draw lymphocytes and a
monocyte.


-
Lymphocytes
-
These cells are very variable in size. The smallest may be
smaller than erythrocytes (down to about 5 µm in diameter)
while the largest may reach the size of large granulocytes (up to
15 µm in diameter). How much cytoplasm is discernible depends
very much on the size of the lymphocyte. In small ones (the
majority of lymphocytes in the blood) the nucleus may appear to
fill the entire cell. Large lymphocytes have a wider rim of
cytoplasm which surrounds the nucleus. Both
the nucleus and the cytoplasm stain blue (and darker than most
other cell types in the blood). The typical lymphocyte only
contains the usual complement of cellular organelles. The
appearance of lymphocytes may change drastically when they are
activated (see below).
Functions
Most lymphocytes in the blood stream belong to either the group
of B-lymphocytes (about 5%) or the
group of T-lymphocytes (about 90%).
Unless they become activated, the two groups can not easily be
distinguished in the light or electron microscope. Upon exposure to
antigens by antigen-presenting cells (e.g. macrophages) and
T-helper cells (one special group of T-lymphocytes) B-lymphocytes differentiate into antibody producing
plasma cells. The amount of
cytoplasm increases and RER fills a large portion of it.
T-lymphocytes represent the "cellular arm" of the immune response
(cytotoxic T cells) and may attack foreign cells, cancer cells and
cells infected by e.g. a virus.
As you may have noticed T-lymphocytes and
B-lymphocytes do not add up to 100%. Try to find some information
on the small but important remainder (a good textbook will contain
a short section on these cells).
- Thrombocytes (or
blood platelets)
-
Thrombocytes do not contain a
nucleus. Unlike erythrocytes, which also lack a nucleus,
thrombocytes have never been individual nucleated cells but are fragments of the cytoplasm of very large
thrombocyte precursor cells,
megakaryocytes. Like other cells involved in the
formation in blood cells, megakaryocytes are found in the bone
marrow.
Platelets are about 3 µm long but appear somewhat smaller
in the microscope. This is because their cytoplasm is divided into
two zones: and outer hyalomere,
which hardly stains, and an inner
granulomere, which contains bluish staining granules. These granules are usually not individually
visible with the highest magnification on your microscope, and the
granulomere appears more or less homogenously blue. In
addition to different types of vesicles
(i.e. the granules), mitochandria, ribosomes, lysosomes and
a little ER are present in the
thrombocyte granulomere. Different types of vesicles contain either
serotonin
(electron-dense delta granules; few) or compounds important
for blood coagulation (alpha granules - they also contain platelet-derived
growth
factor (PDGF) which may play a role in the repair of damaged
tissue). The hyalomere contains cytoskeletal fibres, which
include actin and myosin.
Functions
Platelets assist in haemostasis, the arrest of bleeding.
Serotonin is a potent vasoconstrictor. The release of serotonin
from thrombocytes, which adhere to the walls of a damaged vessels,
is sufficient to close even small arteries. Thrombocytes, which
come into contact with collagenous fibers in the walls of the
vessel (which are not usually exposed to
the blood stream), swell, become "sticky" and activate other
thrombocytes to undergo the same transformation. This cascade of
events results in the formation of a
platelet plug (or platelet thrombus). Finally, activating
substances are released from the damaged vessel walls and from the
thrombocytes. These substances mediate the conversion of the plasma
protein prothrombin into thrombin. Thrombin
catalyzes the conversion of fibrinogen into fibrin, which
polymerizes into fibrils and forms a fibrous net in the arising
blood clot. Platelets captured in the fibrin net contract leading
to clot
retraction, which further assists in haemostasis.
Blood coagulation is a fairly complex process, which involves a
large number of other proteins and messenger substances.
Deficiencies in any one of them, either inherited or acquired, will
lead to an impairment of haemostasis.
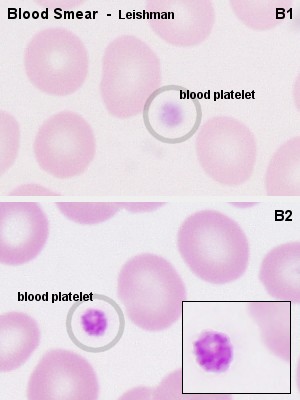 Lab: Slides BLOOD SMEAR LEISHMAN.
In B1, thrombocytes will appear like light blue, fairly ill-defined specks
between the other blood cells. In B2, you will be able to see that the blue
specks are formed by an accumulation of small bluish grains, the granules
of the thrombocytes.
Lab: Slides BLOOD SMEAR LEISHMAN.
In B1, thrombocytes will appear like light blue, fairly ill-defined specks
between the other blood cells. In B2, you will be able to see that the blue
specks are formed by an accumulation of small bluish grains, the granules
of the thrombocytes.
Identify and include a thrombocyte in one of
your other drawings.
Slide GROWING BONE RABBIT H&E.
The marrow cavity of this bone is filled
with red bone marrow. H&E is not the method of choice for
looking at haemopoietic cells, but a few of the numerous named
types or broader groups can actually be recognized.
Precursors of thrombocytes are the haemopoietic cells easiest to
find in red bone marrow. The very dark and large megakaryoblast and
the even larger but light megakaryocytes are clearly visible even
at low magnifications.
Identify and draw a megakaryocyte and
megakaryoblast.


During foetal develoment, the formation of
blood cells commences in wall of the yolk sac. After the second
month of foetal development, the liver, and, slightly later, the
spleen, become the dominant sites of haemopoiesis.
From the 6th month, and dominating from the 7th month onwards,
the formation of blood cells (haemopoiesis) occurs in bone marrow, which is
the major site of formation blood cells in normal adult humans.
Haemopoiesis occurs in red bone
marrow, which is typically found between the trabeculae of
spongy bone. Yellow bone marrow, which harbours mainly adipocytes,
dominates in the hollow of the diaphysis of adult long bones. Both
age and demands on haemopoiesis may effect the relative amounts of
red and yellow bone marrow. Haemopoietic cells surround the
vascular sinusoids and are supported by reticular connective
tissue. In addition to the endothelial cells of the sinusoids and
the reticulocytes of the connective tissue, macrophages are
frequent in red bone marrow.
Haemopoietic Cells
The basis of haemopoiesis is a small population of self-replicating stem cells, which ultimately can generate
all types of blood cells. Their progeny may develop into either lymphocytic
stem cells or pluripotent haemal stem cells
(colony-forming unit - stem
cell - CFU-S). The latter type gives rise to yet another set of stem
cells which form the major groups of blood cells other than lymphocytes. Depending on their progeny it is possible to differentiate
-
burst-forming unit of the
erythroid line (BFU-E)
-
colony-forming unit -
granulocytes and macrophages
(CFU-G/M)
-
colony-forming unit -
megakaryocytes (CFU-Mk)
- Erythrocytes
- The first identifiable stage of erythropoiesis is the proerythroblast - a large, slightly basophilic cell,
which contains a large, lightly stained nulceus. Proerythroblasts proliferate
to generate a sequence of cells which show a gradual decrease in size and
condensation of their chromatin. They are named
after changes in the staining characteristic of their cytoplasm (basophilic
eythroblast, polychromatophilic and orthochromic normoblasts).
The nucleus of the normoblast is finally extruded from the cell.
The cell enters circulation as a reticulocyte,
which still contains some organelles. Reticulocytes remain for a few days
in either the bone marrow or the spleen to mature to erythrocytes.
- Granulocytes
- Myeloblast appear light-microscopically
similar to proerythroblast. They proliferate to generate promyelocytes.
Promyelocytes begin to accumulate non-specific granules, but they are still
able to divide. The maturation of their progeny, the myelocytes,
is characterised by the accumulation of specific granules and changes in
nuclear morphology. Metamyelocytes have a
C-shaped nucleus.
- Thrombocytes
- are, as mentioned above, fragments of the cytoplasm of megakaryocytes.
Megakaryocytes are very large cells (up to 160 µm), which contain
very large, highly lobulated, polyploid nuclei. Megakaryocytes are in turn
the product of the differentiation of basophilic megakaryoblasts.
Precursors of blood
cells which are usually only found in the bone marrow can be found
in peripheral blood in a variety of pathological
conditions.
If a Rh-negative mother has been immunised by erythrocytes
of a Rh-positive foetus, a condition called Erythroblastosis fetalis may develop during subsequent
pregnancies. It would show itself in the foetus or newborn by the presence
of erythrocyte precursors in peripheral blood - although other, more severe
symptoms should be obvious. Chronic myeloid leukemia is another condition
- in this case showing itself by the presence of all types of granulocyte
precursors in peripheral blood.
The nomenclature employed for haemopoietic
cells (but not the number of stages recognized) is somehwat
variable across texts. Note also that these cell types refer to
stages of development along a morphologically more or less
continuous spectrum.
Lab: Slide
GROWING BONE RABBIT H&E. Most of the haemopoietic cells visible will be of
the erythroblastic line, of which we only can easily identify one
broad group of cells. A very condensed nucleus is seen in
late (orthochromic) normoblast.
Granulocyte and erythrocyte precursors will mostly intermingle, but
may be distinguished by nuclear morphology and/or size. A bent
nucleus is found in metamyelocytes - this shape is very pronounced
in the last, immature form of neurophils, which are also called
stab or band cells. If the cell (1) is large, with a distinct
"clearing" in the otherwise pink cytoplasm and (2) has an ovoid or
slightly indented nucleus, it is likely to be a myelocyte. Most
myelocytes/metamyelocytes will give rise to eosinophils. Cells with
large light nuclei and almost unstained cytoplasm are either
reticulocytes or macrophages. Macrophages
are frequently associated with normoblasts, and together these
cells form erythroblastic islands. The name for macrophages in
these islands, nurse cells, may tell you a bit about their function
in addition to the scavenging of the expelled nuclei.
Identify normoblasts, myelocytes and
metamyelocytes and include them in your drawing of the
megakaryocyte/blast.
If you still have some time and are desparate
to get frustrated try to hunt up a nice basophilic erythroblast - a
basophilic cell with homogenously staining nucleus that is somewhat
smaller than the nuclei of granulocyte-precursors.

